A project into appropriate rivastigmine prescribing
Purpose
It is considered best practice that when a healthcare professional is considering prescribing rivastigmine, that patient should have a routine ECG first. If a significant conduction abnormality or prolonged QTc is found then rivastigmine may increase the risk of cardiac conductive /QTc abnormalities and therefore an alternative treatment is desirable.
The author found that in clinical practice the above guidelines were generally, but not always, followed. There also seemed to be no consensus view in the literature or on discussion with colleagues whether the ECG should be routinely repeated during the treatment course or if a repeat ECG was desirable if a dose adjustment was made.
rivastigmine is a medication which is routinely prescribed in our specialist movement disorder clinic. This audit was performed in order to ascertain what practice takes place in our clinic.
Methodology
This was a retrospective case note analysis. The time period studied was August to October 2017.
Cases where the patient was prescribed, had been prescribed or had been considered for rivastigmine where identified by the Parkinson’s Disease Specialist Nurse. The case notes were then examined by myself.
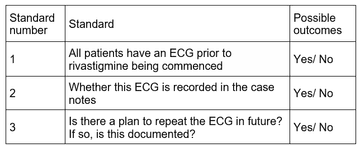
The standards that were aspired to are listed below in Table 1:
The results were analysed using descriptive statistics.
Results
In the studied period, 20 patients where identified as being on or had been considered for rivastigmine.
In one instance, the relevant case notes could not be found, thus the number in the analysis was 19.
Of these patients, 11 had been commenced on rivastigmine prior to clinic referral (58%).
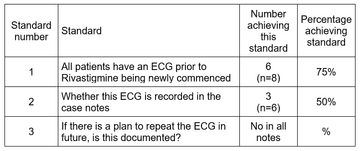
Table 2 – showing if standard we’re meet for the patients that we newly commenced on rivastigmine in clinic.
Discussion
There are clear guidelines about the requirement for an initial ECG in those patients starting rivastigmine. Was is less clear is if there is a necessity for repeated ECGs when dose adjustments are considered or made.
Overall, practice and adherence to guidelines was good. Most patients who were newly prescribed rivastigmine from our clinic had at least one baseline ECG. In some patients, the ECG was performed but there was no subsequent documentation in the medical notes. This is a function of suboptimal record keeping rather than a reflection on clinical practice.
In cases where a dose change was being considered, no instances of repeated ECG were seen.
The other problem the author encountered was in relation to QTc measurement. Older ECGs (from several years ago), did not have automatically calculated QTcs. This meant that colleagues either had to manually calculate the QTc, or assume that it was okay based on a gross visual inspection of the ECG.
In all but one patient the QTc was not prolonged. In this patient, amantadine utilised as second-line treatment.
The author gathered all the notes to the best of their ability, but for some patients there was no access to previous volumes of notes which may have yealded more positive findings.
Conclusions
Guidance on and adherence to guidelines is well done, but further clarification is needed in relation to repeating ECGs in those with dose adjustments. Following this project, a departmental meeting took place. Here it was decided that only if the patient had a history of cardiac disease /was at high cardiac risk, a repeat ECG was necessary.
It was also felt that an aide memoir/rivastigmine initiation proforma would facilitate good record keeping. Hence a proforma was created (see appendix 1.). This will be utilised in the clinic going forward. It will be placed in the notes and should raise compliance with the checking of ecgs and facilitate future data collection.
The completion of this audit has helped to raise awareness in the department about the importance this aspect of safe prescribing of rivastigmine. We intend on re-auditing this once the above has been implemented.
Limitations of the study
This study only looked at very small number of patients case notes and thus it is difficult to know if its findings are representative of the whole population. However, due to the very time consuming nature of the retrospective case note analysis (taking 4 hours to review the 20 sets of notes) and in the interest of pragmatism, the author has distilled conclusions from the currently available information.
Recommendations
The following recommendations will be made in order to try and improve practice:
- Ensure that an ECG is performed in all those patients who have been started on, or who may be started on rivastigmine
- The results of the ECG are to be documented in the case notes using the developed proforma (see Appendix 1)
- In patients whose rivastigmine dose is to be increased and who are deemed high risk, a repeat ECG should be performed and documented in the case notes
- A re-audit is completed once the above recommendations have been implemented
References
- Yorkshire and Humber Clinical Networks. The Assessment of Cardiac Status Before Prescribing Acetyl Cholinesterase Inhibitors for Dementia. April 2016. Accessed 15th November 2017
More Parkinson's Academy Medication Projects

'The things you can't get from the books'
Parkinson's Academy, our original and longest running Academy, houses 20 years of inspirational projects, resources, and evidence for improving outcomes for people with Parkinson's. Led by co-founder and educational director Dr Peter Fletcher, the Academy has a truly collegiate feel and prides itself on delivering 'the things you can't get from books' - a practical learning model which inspires all Neurology Academy courses.